Introduction
Coenzyme Q 10 (CoQ 10) is a Nobel prize winning moiety. It is found in every cell in the human body, hence it is also called ubiquinone (UQ10) (ubiquitous) It forms part of cell membranes and belongs to a class of compounds known as the benzoquinones.
Biochemically, it is a fat soluble molecule which plays two essential functions in the human body:
it acts as an electron carrier in mitochondria which helps convert food to energy
and
it is a powerful anti-oxidant which protects the body against free radical damage.
CoQ10 is currently marketed and promoted as both a nutraceutical and as a cosmeceutical. Just because something has won a Nobel Prize does not necessarily mean that it has to be on my weekly shopping list. What does the scientific literature have to say about CoQ10?
What Is CoQ10?
CoQ was discovered in 1957. Like many important scientific discoveries, it was discovered simultaneously by separate investigators - Drs Festenstein and Morton at the University of Liverpool (who called it ubiquinone) and by Dr Fred Crane at the University of Wisconsin (who called it Coenzyme Q).
British scientist Peter Mitchell won a Nobel Prize in 1978 for his work on the mechanism of action of CoQ in transferring energy in the body.
CoQ is necessary for cellular production of adenosine triphosphate (ATP) which is the basic building block of energy in human cells.
It also neutralises the harmful effects of free radicals generated by mitochondria.
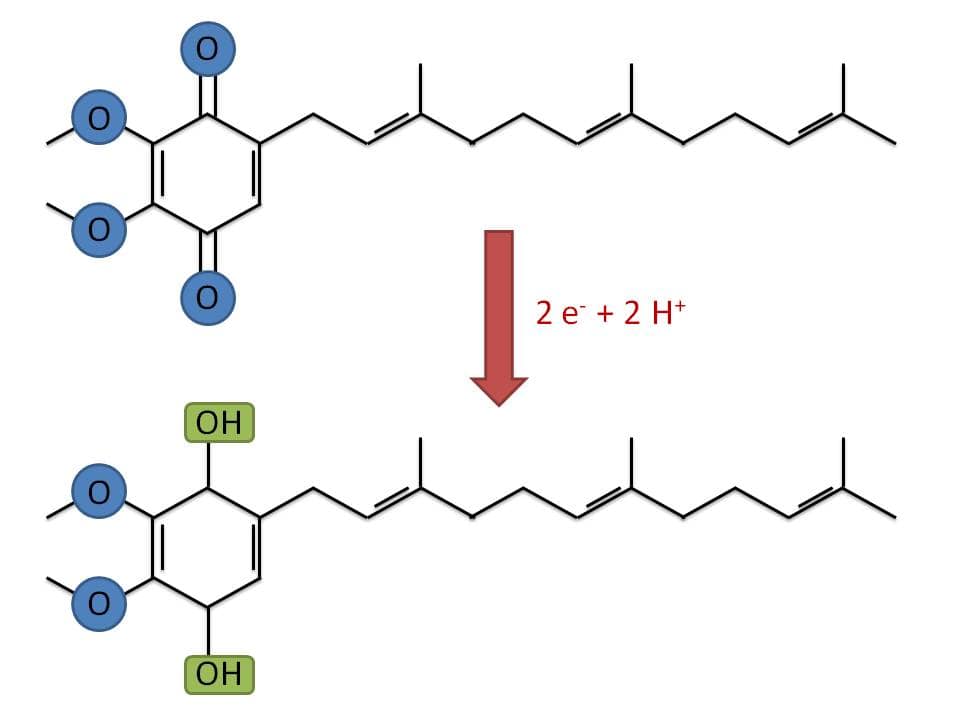
CoQ is a 1,4 benzoquinone where Q refers to the quinone chemical group and 10 refers to the number of isopropyl chemical subunits in the tail. It is a co-enzyme which means it is an enzyme helper to help other enzymes to help then do their work better. Enzymes are catalysts that accelerate biochemical reactions. (All very biochemical I know, but helpful to understand the odd nomenclature).
CoQ is universally present in the phospholipid bilayer of human cell membranes but is best studied and understood in the mitochondria. CoQ is found in the mitochondria of all cells in the human body (mitochondria are the energy power plants for humans). Red blood cells have no mitochondria but most other human cells have mitochondria.
Emerging research is focusing on the role of CoQ in membranes other than mitochondria such as the Golgi apparatus (1). The Golgi apparatus is involved in protein modification and export.
CoQ is the only lipid soluble antioxidant that animal cells can synthesize de novo. All cells can synthesize CoQ under normal physiological conditions but this ability wanes over time. Metabolically active cells (heart, liver and kidneys) have the highest requirement for and content of CoQ.
CoQ exists in three states:
- fully oxidized ubiquinone
- semi-oxidized semi-quinone
- fully reduced (the useful anti-oxidant form) ubiquinol.
Ubiquinone is the form of CoQ that is involved in energy generation via the ATP pathway while ubiquinol is the form that acts as an antioxidant which neutralizes reactive oxygen species (this distinction becomes important later when we look at different CoQ formulations).
The bioavailability (F%) of CoQ is very low at just 6% which means that only 6% of ingested CoQ actually reaches the systemic circulation (again this is important when it comes to CoQ supplementation).
There are over 7000 CoQ10 products for sale on Amazon which includes capsules, powders, serums and anti-ageing creams. CoQ is sold alone and in combination with other agents e.g. with EPA and DHA in supplement capsules or with hyaluronic acid in anti-ageing creams.
The typical cost of a 100 mg capsule of CoQ is about $0.15.
Can You Get CoQ10 From Food?

Primary deficiency of this molecule is very rare e.g the autosomal recessive Leigh syndrome. Secondary deficiencies of CoQ can occur with hydroxymethylglutaryl coenzyme A (HMG CoA) reductase inhibitors more commonly known as statins. Secondary deficiencies are also seen with beta-blockers, anti-hypertensive medications and tricyclic anti-depressants.
There are no specific dietary intake recommendations for CoQ (there must be a reason for this?). The average daily intake of CoQ from diet is low at 3-6mg with only about half of this being in the reduced state (ubiquinol).
Meat, poultry and fish are relatively rich sources of CoQ followed by soybeans, canola oils and nuts. Not all meat is created equally when it comes to CoQ10. As mentioned above, tissues such as heart and kidney are naturally rich in CoQ and animal sources of heart and kidney are the best food sources of CoQ10. Fruits, vegetables and eggs and dairy are only moderate sources of CoQ10.
Between 14 and 32% of CoQ10 is destroyed by the process of frying vegetables and eggs. Boiling has a lesser effect on the content of CoQ in foods.
Here are the typical expected CoQ 10 content of common foods:
- Beef (3oz) 2.6mg
- Herring three (3oz) 2.3 mg
- Chicken (3oz) 1.4 mg
- Boiled egg (medium) 0.1 mg (2).
- Work is underway to try to fortify foods with CoQ. This is being done by increasing the CoQ content in animal feeds and by
- genetic modification of cereals.
Genetically modified gram negative bacteria such as E. coli are being studied in attempts to increase the production of CoQ for commercial purposes (3).
CoQ is fat soluble and should be taken with food containing some fat in order to improve absorption.The absorption of CoQ from soft gels is generally superior to other formulations such as capsules.
The question still remains as to whether we need to consider high COQ10 containing foods or CoQ supplementation in the first place?
Is There Any Research?
There are 16000 published studies on CoQ which includes over 1000 human clinical trials. This is pretty impressive considering the fact that we only know of its existence for 60 years. Let’s compare CoQ to arginine which has a similar number of publications, clinical trials and even a Nobel Prize to boost of. The big difference here is that arginine was discovered way back in 1895.
Does CoQ10 Improve Energy?
CoQ is critical to cellular production of ATP. This does not necessarily mean that CoQ contributes to our overall feeling of energy and vitality.
CoQ has been shown to improve exercise tolerance in a select subset of patients with mitochondrial encephalopathies (4) . But what about the general population?
Seven placebo controlled trials looked at supplementation with CoQ (100-150mg/day) and found no difference between the groups in terms of maximal oxygen production (VO2 max) and exercise time to exhaustion. As an example, Australian researchers studied the effect of orally supplemented coenzyme Q10 on plasma CoQ10 concentration and aerobic capacity in endurance athletes (5).
A total of 18 volunteers were assigned to either CoQ or placebo. Plasma CoQ levels increased in the treatment arm of the study but the CoQ10 supplementation regime had no consistently significant effect on oxygen uptake, anaerobic and respiratory compensation thresholds, blood lactate, glucose and triglyceride kinetics, heart rate, and blood pressure during and after graded cycling to exhaustion.
Some studies actually showed that placebo was better than CoQ in terms of exercise tolerance. As an example Swedish investigators carried out a placebo controlled trial in 18 subjects who received either placebo or CoQ over 22 days (6). The results demonstrated, that on an anaerobic (10 x 10 s) cycling test, the placebo group showed a significantly greater improvement than the Q10-group after a supplementation and training period (P < 0.001).
There was no significant difference between the groups, either in VO2max (maximal volume of 02 delivered to the tissues per minute) determined during running, or in sub maximal and peak VO2, rate of perceived exertion, respiratory quotient, blood lactate concentration or heart rate determined during sub maximal and maximal cycling.
Bottom line
CoQ has not been shown to improve energy in the general population.
Does It Reduce Free Radical Damage?
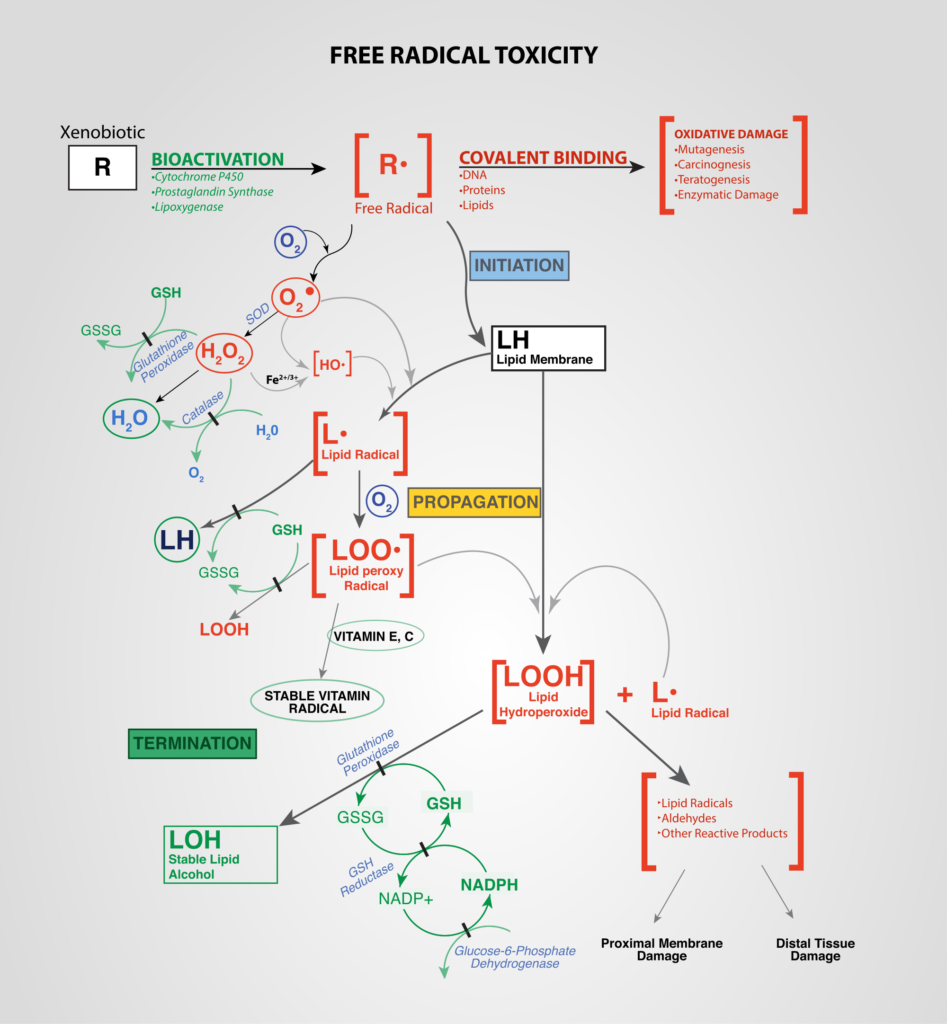
Free radicals are reactive chemical species having a single unpaired electron in the outer orbit. Free radicals induce oxidative stress which needs to be balanced/offset by the body’s endogenous antioxidant systems. There is a complex interplay between free radicals and antioxidants.
Disturbance of this balance results in oxidative damage which is believed to contribute to age dependent diseases such as cardiovascular disease, cancer, neurodegenerative disorders and other chronic conditions. Mitochondria are the major site of free radical generation. Mitochondria contain a variety of antioxidants present on both sides of their membranes in order to minimize reactive oxygen species induced stress.
CoQ is the main antioxidant in the mitochondrial membrane. This means that functionally CoQ is designed to reduce free radical damage. There are no clinical trials looking at the effects of CoQ on the direct effects of CoQ on free radical damage. There are studies looking at the downstream effects of free radical damage which we will review in the next sections.
Bottom line
CoQ is designed to reduce free radical damage and there are no specific studies looking at the clinical effects of CoQ on the reduction of free radical damage.
Does It Improve Heart Health? Reduce Effects Of Statin Drugs?
There are almost 2000 published studies on CoQ and cardiac health.
Researchers from Case Western did a Cochrane review of CoQ for heart failure (7). They analysed data from 7 published randomised trials (914 study participants) which compared CoQ to placebo in patients with heart failure. Pooled analysis showed that no conclusions can be drawn on the benefits or harms of CoQ in heart failure at this time due the fact that there are only a limited number of small studies with very different designs and methodologies.
Another Cochrane review looked at blood pressure lowering effect of CoQ (8). Researchers from British Colombia, Vancouver identified just two clinical trials (50 participants) which met the criteria of being randomized placebo controlled clinical trials of at least three weeks duration that studied CoQ versus placebo in patients with primary hypertension. The review provided moderate quality evidence that CoQ does not have a clinically significant effect on blood pressure.
A third Cochrane review from the University of Warwick looked at the role of CoQ in the primary prevention of heart disease (9). They found four trials which investigated CoQ10 supplementation in patients on statin therapy. Three of the studies showed that simultaneous administration of CoQ10 did not significantly influence lipid levels or systolic blood pressure levels between the two groups.
The fourth trial showed a significant increase in the change in total and low-density lipoprotein (LDL)-cholesterol at three months across the four arms of the trial (α-tocopherol, CoQ10, CoQ10 + α-tocopherol and placebo), however the way in which the data were presented meant that they were unable to determine if there was any significant difference between the CoQ10 only and placebo arms.
Secondary deficiencies of CoQ can occur with hydroxymethylglutaryl coenzyme A (HMG CoA) reductase inhibitors more commonly known as statins. Researchers from the UK did a meta-analysis of available randomized controlled trials but did not find evidence to suggest any significant benefit of CoQ10 supplementation in improving statin-induced myopathy. Larger, well-designed trials are necessary to confirm the findings from this meta-analysis.(10).
Finally, CoQ is being studied for potential benefit for patients undergoing cardiac surgery (11). In a randomized, clinical trial, 100 Iranian patients who were scheduled for elective percutaneous coronary intervention were allocated in to the intervention (n=50) and control group (n=50). The intervention received a 300 mg loading dose CoQ10 12 hours before procedure.
The results showed that pretreatment with 300 mg CoQ10 12 hours before procedure could not reduce Periprocedural myocardial injury following elective percutaneous coronary intervention, however, significantly decreased CRP (a marker of inflammation).
Bottom line
CoQ levels are relatively higher in cardiac muscle than other human tissues. It is widely believed that CoQ helps cardiac health. It is certainly possible to selectively read the medical literature and quote the positive results of individual studies.
However available meta-analyses do not support a role for CoQ in cardiac health. This may be due to two reasons: either CoQ does not work or it does work but the studies are not well enough designed to show it.
Does it Slow The Effects Of Ageing?

The oxidative stress hypothesis of ageing states that the level of ‘oxidant load or stress’ increases during ageing, and plays a causal role in senescence (much like rusting). Reactive oxygen species are generated by mitochondria as a byproduct of ATP production. Reactive oxygen species may damage mitochondria over time, causing them to function less efficiently and to generate more damaging ROS in a self-perpetuating cycle.
Coenzyme Q10 plays an important role in mitochondrial ATP synthesis and functions as an antioxidant in mitochondrial membranes. A decrease in endogenous CoQ synthesis occurs with the natural ageing process (12). This does not necessarily mean that CoQ supplementation is an anti-ageing sine qua non.
Investigators from the University of Granda, Spain assigned 32 male rats to either CoQ supplementation or nothing. Eight rats in each group were killed at 6 and 24 months. As an FYI, one human year is equivalent to approximately equal to 14 rat days (13). There was no placebo arm of the study. I had never thought about this until now. Do rats experience a placebo effect?
(Please forgive the detour but I simply had to know? Feel free to skip ahead if your interest is not piqued. There is a study which showed that administration of injectable placebos may have an affect on rats (14). The study showed that the immobility time in the despair test was higher in the placebo-treated rats than in untreated intact controls. Technically this is not a placebo response but a nocebo but it certainly raises questions about the need for placebo arms in rat studies.)
Anyway back to CoQ!
The longterm supplementation of rats with CoQ attenuated age related reductions in antioxidant capacity and age related increases in DNA damage in peripheral blood lymphocytes. We have to remember that rats are not miniature humans and great care needs to be taken anytime we try to extrapolate or correlate rat and human data.
A comprehensive review of the role of CoQ in the dietary therapy of ageing was published in the journal Molecules in 2016 (15). The article listed the various anti-ageing mechanisms of CoQ including:
- cell bioenergetics
- antioxidation
- anti-inflammatory
- and prevention of programmed cell death.
The authors summarised the results of clinical studies in this single statement
‘Due to differences in dosage, duration, chemical formulation and subject age at the beginning of the treatment, it is very difficult to establish “ideal conditions” for CoQ use as “anti-ageing therapy”.
Bottom line
There is no science to support a clear role or prescriptive strategy for CoQ supplementation as an anti-ageing strategy.
Does It Help Maintain Optimum PH Levels?
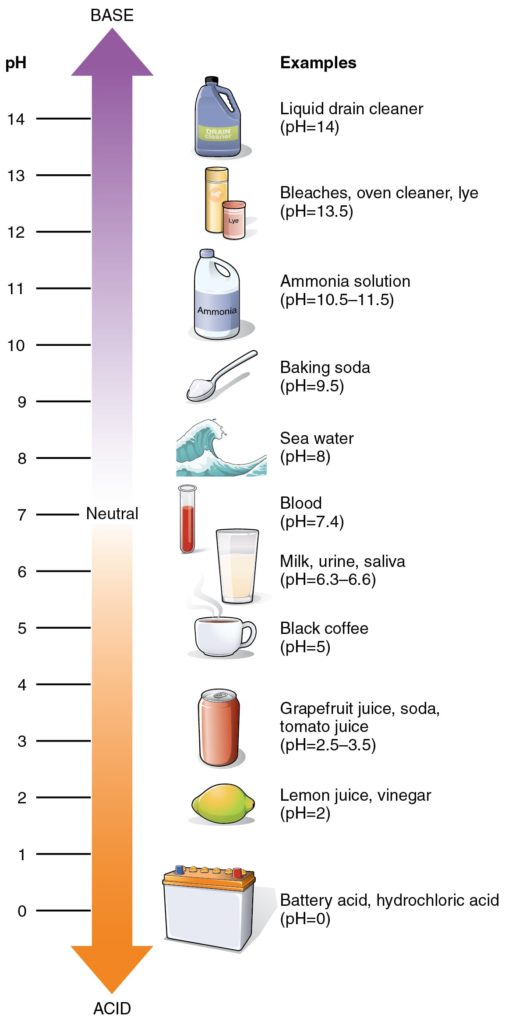
CoQ transfers hydrogen ions from the cell cytosol to inside the cellular lysozyme. Lysozymes are intracellular organelles that play a role in the elimination of unwanted materials form cells ( I must contact Marie Kondo to suggest a new bestselling book for her ‘The Life Changing Magic of Lysozymes’). This contributes to the maintenance of an acidic pH in the lysozyme (16). There is nothing to suggest that this plays any role in the overall pH of the body.
Bottom Line
CoQ helps maintain optimum pH in lysosomes but this does not imply that it affects overall body pH.
Does It Affect The Brain or Cognition?

Again this question follows the general theme of the role of CoQ as an anti-ageing agent. There are two studies which are worthy of mention here.
A study in mice found that prolonged intake of low dose CoQ10 in low amounts (0.68 mg/g) had no discernible impact on cognitive and motor functions whereas intake at higher amounts (2.6 mg/g) exacerbated cognitive and sensory impairments encountered in old mice (17). Oops.
A phase III randomized, placebo-controlled, double-blind clinical trial at 67 North American sites consisting of participants 30 years of age or older who received a diagnosis of Parkinson’s Disease within 5 years (18). The study was funded by the National Institutes of Health. A total of 600 participants were randomly assigned to receive placebo, 1200 mg/d of CoQ10, or 2400 mg/d of CoQ10; all participants received 1200 IU/d of vitamin E. The futility analysis used a predictive power criterion so that an active treatment arm would be terminated if the likelihood of its demonstrating a statistically significant benefit over placebo was less than 10%. The study was terminated after the pre specified futility criterion was reached.
Coenzyme Q10 was safe and well tolerated in this population, but showed no evidence of clinical benefit.
Bottom line
There is no conclusive evidence that CoQ supplementation will benefit brain function.
Does CoQ help Gulf War Syndrome?

Investigators in San Diego evaluated CoQ10 in 46 veterans with confirmed Gulf War Illness (19). The veterans were randomized to either CoQ 100mg or CoQ 300mg or placebo for four months.
In conclusion, CoQ conferred benefit to physical function and symptoms (except sleep) in veterans with Gulf War illness.
Bottom line
There is some preliminary data to suggest that CoQ is worth studying in veterans with Gulf War syndrome.
Does CoQ help with male infertility?
Italian researchers evaluated CoQ (100 mg twice daily for six months) in 22 men with reduced sperm motility (20). Significant increases in CoQ levels and sperm motility were noted. The researchers concluded that CoQ may play a role in asthenozoospermia (sperm with reduced motility).
Bottom line
A small single study provides positive proof of concept that CoQ is a worthy candidate for future male infertility studies.
Ubiquinol versus Ubiquinone?
In 2006, a CoQ supplement containing CoQ in its reduced form (ubiquinol) was launched. Clinical researchers questioned the marketing claims for this new product by pointing out that it was ‘factually but not functionally’ important’ for the following reasons:
- All studies on CoQ focus on the oxidised ubiquinone form.
- Like all anti-oxidants, ubiquinol is unstable.
- Ubiquinol is converted to ubiquinone in the lumen of the stomach and small intestine and then converted into back to ubiquinol once it is absorbed ( so an unnecessary merry-go-round essentially)
Oh did I mention that ubiquinol products are more expensive than ubiquinone?
Is CoQ10 Supplementation Safe?
Canadian investigators evaluated the effect of CoQ in 28 subjects over 20 weeks in an open label trial design. Subjects included 20 patients with Huntington's Korea and eight healthy volunteers. The study participants started at a dose of 1200 mg of CoQ per day and increased by 1200 mg every four weeks to a maximum dose of 3600 mg per day.
A total of 23 subjects (82%) achieved the target dose of 3600mg per day. The most common adverse events noted related to the gastrointestinal tract and six subjects withdrew due to gastrointestinal toxicity. Main gastrointestinal symptoms include nausea, diarrhea, appetite suppression, heartburn, and abdominal discomfort.
CoQ plasma levels were also measured. CoQ levels were
1.26+/- 1.27 µg/ml at baseline
5.59 +/- 2.24 µg/ml at 1200mg/day
6.38 +/- 3.25 µg/ml at 2400mg/day
7.49 +/- 4.09 µg/m; at 3600mg/day/
The researchers concluded that doses of 2400mg per day achieve the best balance between tolerability and CoQ blood levels (21).
The safety of CoQ in pregnancy and breastfeeding has not been established. It is advised that pregnant and nursing women should avoid CoQ.
The effects of CoQ in patients receiving chemotherapy are complex and expert advice from an integrative oncologist is required before taking CoQ while on chemotherapy. As CoQ is an antioxidant it may reduce the effects of some chemotherapy agents. On the other hand CoQ may reduce the cardiac toxicity of two commonly used chemotherapeutic agents doxorubicin and daunorubicin. Complex and you definitely don’t want to get this wrong.
CoQ may enhance the effect of some antihypertensive medications.
CoQ may exert a hypoglycemic effects and care is advised in patients taking anti-diabetic medications.
Finally, CoQ may reduce the efficacy of blood thinning medications.
Conclusion
CoQ is pretty amazing. It deserves a Nobel Prize as it is a super smart compound. It is the ultimate model of eco-friendly design for energy production.
In a nutshell, it generates energy and cleans up after itself. That being said, having reviewed the data, I see no reason why most people would want to supplement with CoQ.
There are two options for CoQ supplementation: food or supplements. As a vegetarian, you would want to provide me with unequivocal scientific proof of benefit before I would start eating offal (and ideally boiled or raw offal -ugh!).
Equally as a pharmacologist, it is against my religion to buy supplements when I can only absorb 6% (meaning that I would excrete 94% of my money).
Essentially CoQ is mission critical to our survival but we don’t depend on external sources of CoQ a and concentrations of CoQ are ‘tightly distributed around a homeostatic set point’. In other words, nature has this covered.
At this time there is absolutely no proof that CoQ supplementation makes us healthier.
Like I said, CoQ is a super smart designer compound and there is nothing to suggest that we should try to second guess nature on this one.
Nature has this one covered.
Leave a Reply